
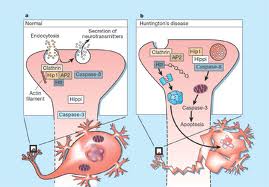
HD results from genetically programmed degeneration of nerve cells, called neurons, in certain areas of the brain. This degeneration causes uncontrolled movements, loss of intellectual faculties, and emotional disturbance. Specifically affected are cells of the basal ganglia, structures deep within the brain that have many important functions, including coordinating movement. Within the basal ganglia, HD especially targets neurons of the striatum, particularly those in the caudate nuclei and the pallidum. Also affected is the brain's outer surface, or cortex, which controls thought, perception, and memory.
Involves disturbance in neurotransmitter substance primarily: Gamma Aminobyutric Acid (GABA) & Dopamine

GABA neurons in basal ganglia, frontal cortex and cerebellum are destroyed
GABA neurotransmitter production
Excess of dopamine causes abnormal neurotransmission along the affected pathway

Chorea and mental deterioration

Enlargement of the ventricles in HD patients due to atrophy of
the head of the caudate from neuronal loss.
the head of the caudate from neuronal loss.
------------------------------------------------------------------------------------

A rapidly progressive, invariably fatal neurological disease that attacks the nerve cells (neurons) responsible for controlling voluntary muscles. The disease belongs to a group of disorders known as motor neuron diseases, which are characterized by the gradual degeneration and death of motor neurons. Mental status of the patient is intact and not affected.
ALS results from degeneration of:
- upper motor neurons in the medulla oblongata
- lower motor neurons in the spinal cord


Muscle atrophy (loss of muscle tone)


------------------------------------------------------------------------------------
PARKINSON'S DISEASE

Parkinson's disease is a brain disorder that causes gradual loss of muscle control. It is a slowly progressing neurologic movement disorder that eventually leads to disability.
WHAT CAUSES PD?

A small area in the brain stem called the substancia nigra controls movement. The cells in this part stops producing dopamine, a chemical that helps nerves to communicate. As these dopamine producing cells die, the brain does not receive the necessary messages about how and when to move.
SIGNS & SYMPTOMS

- Slight shaking of a finger, hand, leg, or lip.
- Stiffness or difficulty in walking.
- Impaired balance.
- Stooped posture.
- A 'masked face', frozen in a serious expression.

-----------------------------------------------------------------------------------
MULTIPLE SCLEROSIS

A disease in which the nerves of the central nervous system degenerate. It affects the pathways of the brain and the spinal cord and results in the destruction of myelin, a covering or insulation for nerves, that improves the conduction of impulses along the nerves and also is important for maintaining the health of the nerves.
WHEN MULTIPLE SCLEROSIS ATTACKS

In multiple sclerosis, an agent such as a virus or foreign antigen, in theory, may alter or interact with the immune system so that the immune system perceives myelin as an intruder and attacks it. Inflammation occurs and causes myelin to disappear. Consequently, the electrical impulses that travel along the nerves decelerate, that is, become slower. In addition, the nerves themselves are damaged. While some of the myelin may be repaired after the assault, some of the nerves are stripped of their myelin covering (become demyelinated). Scarring also occurs, and material is deposited into the scars and forms plaques. As more and more nerves are affected, a person experiences a progressive interference with functions that are controlled by the nervous system such as vision, speech, walking, writing, and memory.
WHAT HAPPENS WHEN THERE IS MULTIPLE SCLEROSIS


-----------------------------------------------------------------------------------
CEPHALALGIA ( HEADACHE )

Pain in the head caused by dilation of cerebral arteries or muscle contractions.

{kind=link}
{kind=link}
results from pressure on
pain receptor (prostaglandin)
 inflammation occurs
inflammation occurs


muscle tension



{kind=link}
EPILEPSY

GROUP OF NEURONS LOSE ITS AFFERENT STIMULATION

{kind=link}
THESE NEURONS ARE HYPERSENSITIVE AND EASILY ACTIVATED
FIRE ABNORMALLY
SEIZURE

INCREASED INTRACRANIAL PRESSURE

Intracranial pressure (ICP) is the pressure in the skull that results from the volume of three essential components: cerebrospinal fluid (CSF), intracranial blood volume and central nervous system tissue. The normal intracranial pressure is between 5-15 mmHg.
{kind=link}
TRAUMA
EDEMA
ICP
BLOOD VESSEL COMPRESSION
{kind=link}
OXYGEN PERFUSION IN THE BRAIN

BRAIN CELL DEATH

MYASTHENIA GRAVIS (MG)
Chronic autoimmune neuromuscular disorder affecting the neurumuscular joint. It is purely a MOTOR Disorder with no effect on sensation or coordination.

- characterized by fatigue and severe weakness of skeletal muscles.
- occurs with remissions and exacerbations.
- occurs more frequently in females, with onset between ages 20-30

- Ptosis (drooping of eyelids), Diplopia (double vision)
- weakness in mouth muscles resulting in dysarthria and dysplagia
- weak voice, smile appears as snarl.
- muscles are weak but DTRs are normal
Pneumonia
Myasthenic crisis
- Sudden exacerbation of motor weakness putting client at risk for respiratory failure and aspiration
- Manifestation: tachycardia, tachypnea, respiratory distress, dysphasia
- Occurs with overdosage of medications (anticholinesterase drugs) used to treat MG
- Develops GI symptoms, severe muscle weakness, vertigo and respiratory distress
- physical examination and history
- Tensilon Test: edrophonium chloride administered and client with myasthenia will show significant improvement lasting 5mins.
- EMG: reduced action potential
- Antiacetylcholine receptor antibody serum levels; increased in 80% MG clients; used to follow course of treatment
- Serum assay of circulating acetylcholine receptor antibodies
- Anticholinesterase medications [pyridostigmine bromide 'Mestinon']
- Immunsuppression medications including glucocorticiods (cyclosporineor azathioprine 'Imuran')
- Teaching interventions to deal with fatigue
- Importance of following medication therapy
- Ineffective airway clearance
- Impaired swallowing: plan to take medication to assist with chewing activity

----------------------------------------------------------------------------------
BELL'S PALSY

The nerve that is injured with Bell's Palsy is CN-VII (7th cranial
nerve). It originates in an area of the brain stem known as the Pons.
The 7th nerve passes through the stylomastoid foramen and enters the
parotid gland. It divides into its main branches inside the parotid
gland. These branches then further divide into 7000 smaller nerve fibers
that reach into the face, neck, salivary glands and the outer ear. The
nerve controls the muscles of the neck, the forehead and facial
expressions, as well as perceived sound volume. It also stimulates
secretions of the lower jaw, the tear glands and the salivary glands in
the front of the mouth. Taste sensations at the front 2/3 of the tongue
and sensations at the outer ear are transmitted by the 7th nerve.
PATHOPHYSIOLOGY
Post infectious demyelination (loss of fatty covering of the nerve coverings called
called myelin sheath) of the facial nerve due to a prior upper respiratory infection
( INFLUENZA )

Inflammation within a small bony tube called the fallopian canal
Pressure is produced on the nerve resulting to its compression
within its bony canal
Inability of the damaged nerve to exit the skull and
divide into its several branches
Impairment of ALL functions controlled by the 7th cranial nerve
Interruption in the transmission of messages
the brain sends to the facial muscles
Idiopathic Facial Paralysis or
BELL'S PALSY
Facial weakness or Paralysis is to one or both sides;
drooping of the eyelid and corner of the mouth; drooling; dryness of the
eye or mouth; impairment of taste; excessive tearing in one eye;
speech difficulties and inabilityto eat on the affected area due to the relaxation of facial muscles
-----------------------------------------------------------------------------------
MENINGITIS
PATHOPHYSIOLOGY
Microorganisms
/ \
/ \
Direct to CSF Via BLOOD

_________________________________________

Subarachnoid space
from Astrocytes+Microglia
Cytokine Release
Increase Blood-Brain Barrier Increase number of WBC in CSF Vasculitis of Cerebral vessels
Permeability
Fluid leakage from vessels Inflammation of Meninges Decrease cerebral blood flow
Vasogenic edema Interstitial Edema Ischemia,cytotoxic edema
(increase ECE)
Cerebral Edema
Decrease Cerebral Blood Flow, Ischemia, Apoptesis (BRAIN DEATH)
